
Buffy and Ernie Goodban watched helplessly for months as a mood disorder took control of their 14-year-old daughter Andrea.
In March, she flooded the family’s North Carolina home, causing more than $40,000 in damage. But more importantly, her mother said, “She was hurting her brothers; she was threatening to harm herself. One day, she ran for the scissors as she was saying she was going to cut her wrists.”
That’s when the Goodbans rushed Andrea to the nearest emergency room, and that’s when they learned about boarding.
Instead of turning the Goodbans and their daughter away, the family said the hospital she was rushed to chose to board her, meaning she was allowed to stay at the hospital until a bed for adolescent psychiatric patients became available somewhere in the state. The hospital couldn’t treat her because it doesn’t have an adolescent psychiatric unit.
“From the get-go, they told me they may not be able to find a place,” Buffy Goodban recalled. “They told me right away, it’s very difficult to find a bed.”
And it was. Days of boarding turned into weeks.
Andrea began her wait in the emergency department but eventually was moved to the pediatric unit. “She wasn’t getting any kind of therapy, counseling programs,” her father said. “Nothing.”
The Goodbans had fallen victim to an overtaxed, fragmented mental health system that is especially short on beds, staffing and outpatient treatment for young mentally ill patients. It often results in the sickest children waiting hours, days or, as was the case with Andrea, weeks before they are admitted to a facility that can provide the specialized care they need — and spending the entire time in an emergency department is not unusual.
A Scripps News investigation reveals that psychiatric boarding doesn’t discriminate by families’ race, income or whether they are insured, and there are no geographic exceptions. It’s a nationwide problem.
Boarding in the emergency room isn’t unusual for patients waiting for other types of treatment, but hospitals report mentally ill patients are boarded most frequently. Doctors and nurses said the long waits could be traumatizing for young psychiatric patients.
“Children are not meant to be confined in a space where they don’t have distractions or education or resources to help them get better,” said Dr. Jane Brice, who chairs the Emergency Medicine Department at the University of North Carolina. “Adults can process that and understand it a little better … children don’t have that capacity.”
Most hospitals don’t keep track of the number of children who board at their facility, but some do. At Children’s National Medical Center in Washington, D.C., a hospital spokesperson told Scripps News that 100 children were stuck boarding there in 2015, up from 65 the year before. Phoenix Children’s Hospital reported that 225 children were boarded there in 2015, often for more than 24 hours, and San Diego’s Rady Children’s Hospital reported that each month some children board for longer than 72 hours in the emergency department before being admitted.
Scripps News surveyed more than 600 child and adolescent mental health care facilities nationwide about boarding, and 203 responded to at least some of the questions. To a question that received 118 responses, 105 facilities reported having to refer children elsewhere last year because their beds were full.
Boarding is “one of the scariest things you’ll ever have to go through,” said Erica Sarro of Saugus, Mass., whose 16-year-old son Jonathan has boarded countless times.
“They just take you out in the hallway and they say, ‘Listen, your child needs a bed. But it’s Friday; you’re not going to get a bed. So be prepared. You might want to tell your husband to find day care for the other kids.’”
In many cases, boarded children wait in a hospital unit where staff members lack training in child or adolescent psychiatry, which is what happened to Andrea Goodban.
It also is what happened to Linette Murphy’s 14-year-old daughter Sapphira, who has been diagnosed with disruptive mood dysregulation disorder, a condition that leads to extreme irritability and intense outbursts. One morning, Sapphira attacked her mother while she slept.
No hospital in Massachusetts had room in its child psychiatric unit, so Sapphira was boarded on a hospital’s neurology floor instead.
“It’s not a mental health facility, so there aren’t people to treat (her),” Murphy said. “So my mom and I were there the whole time … we were the mental health professionals.”
While she waited in a private room, Sapphira went into the bathroom, locked the door and swallowed a washcloth.
“She was throwing up and aspirating,” recalled Murphy, who watched as hospital staff struggled to remove the cloth from her daughter’s throat. “They had to make the decision: Do we continue to get bit and injured from this child, or do we let her aspirate and revive her after?”
Sapphira recovered, but finding a hospital to admit her became more difficult. While she continued to board, a hospital staffer contacted facilities along the northeast coast. In an e-mail Murphy shared with Scripps News, the staffer reported that 16 facilities from Massachusetts to Maine were not able to admit her.
In most cases, it was due to a lack of space. But sometimes, Murphy said, it was because hospitals deemed Sapphira too aggressive.
Some hospitals classify children like Sapphira as “too acute,” meaning they could present a danger to staff or other patients already admitted. That can result in the most severely ill children waiting the longest — and traveling the farthest — to find a bed.
In Sapphira’s case, after waiting for 21 days, she was finally admitted to a mental health facility 96 miles from her home.
The Scripps News survey provided a gauge of how difficult it can be for facilities at capacity to place children and adolescents in a nearby suitable treatment center. Of 113 facilities that responded, 57 reported having to refer children to hospitals more than an hour away.
“We call it reverse triage,” said Kate Ginnis, director of mental health policy for Boston Children’s Hospital. “The concept of triage is that you do the first things first, and the first things are anything life threatening.” But that’s not true with psychiatry, she said. The sickest patients often don’t get admitted and treated before patients with less severe conditions.
Ginnis is part of a group of mental health professionals studying the boarding problem in Massachusetts, which has struggled for years to meet the demand for child psychiatric beds.
While a lack of inpatient beds has contributed to the longer waits, Ginnis said it is only one of many factors. For example, while child psychiatric beds are full for most of the year, many hospitals actually see a lull in admissions during the summer when children are out of school and under less stress. Of 122 facilities that responded to questions about peak admission times, 108 reported that demand for beds is highest during the school year.
The seasonality of the problem, Ginnis said, makes it difficult for some facilities to justify increasing the number of beds and staff if they know admission rates will be lower from June through early September.
Also making hospitals more hesitant to expand services, experts say, is the fact that reimbursement rates for providing child or adolescent psychiatric care sometimes leave hospitals in the red. More complex cases require more staff and usually mean higher costs, but the reimbursement rates negotiated by most insurance companies are sometimes not enough to cover a hospital’s expenses.
“It can be challenging for the units to be able to provide appropriate, safe care and, frankly, stay in business,” Ginnis said.
Dr. Henry Sachs, chief medical officer at Bradley Hospital in Riverside, R.I., puts it more bluntly.
“It’s not a good business model,” he said. “If you went to a bunch of investment bankers and said here’s a business model for a child psychiatry line of business, they would kind of laugh.”
Sachs’ hospital is rare. All 70 of its beds are devoted to the treatment of children and adolescents in need of acute psychiatric care. Beginning in 2011, the hospital saw demand increase sharply, leading to frequent boarding. The problem persisted and, by 2014, Bradley and its sister facility, Hasbro Hospital, saw a record 502 children boarding.
Faced with the opportunity to add more beds, Sachs chose instead to address what he saw as a gaping hole in the outpatient care available to children in Rhode Island.
He and his team created partial-hospitalization programs for children who weren’t sick enough to require an overnight inpatient hospital stay, but needed more specialized treatment than they would be able to find elsewhere through outpatient treatment. They also started afterschool programs and invested in in-home services and a crisis line to route families to the most appropriate care setting.
The following year, the number of boarders was cut to 257. This year, Sachs said, the hospitals are on pace to report even fewer.
Still, Sachs isn’t celebrating. Bradley’s success, he cautioned, can’t be easily duplicated by most traditional hospitals that have competing interests.
“The cardiologist, the neurologist, the oncologist, they all want and need growth in their services, too,” Sachs said, adding that the reimbursement rate for all psychiatry usually lags behind most other medical treatments.
“Financially,” Sachs said, “child psychiatry is not the place you would necessarily want to devote the resources.”
For decades, the number of beds for mentally ill patients of all ages in government-funded hospitals has plummeted. In 1970, there were more than 330,000, but by 2010 fewer than 50,000 remained, according to the Treatment Advocacy Center.
Between 2010 and 2014, surveys by the American Hospital Association showed the number of private and public psychiatric beds for both children and adults fell in 33 states.
The shift has come as a result of decades of deinstitutionalization and shifting mental health resources out of hospitals into local communities. But while beds have surely disappeared, experts say, the community resources have been slow to appear.
“We don't have the intensive outpatient children's mental health services that would help avoid the need for emergency room visits,” said Angela Kimball, director of policy at the National Alliance on Mental Illness.
“We hear about cancer wings opening up and hospitals dedicated to serving other disease conditions,” Kimball said. “But when have you heard about a big foundation opening up a brand new psychiatric hospital for children? You don’t hear it.”
It’s not just crisis services that the mental health system lacks. Even finding a child or adolescent psychiatrist can turn into a painful, time-consuming ordeal.
In North Carolina, Elizabeth Dellinger learned that the hard way when she tried to find a psychiatrist for her 5-year-old son Brian, who suffers from a mood disorder that causes him to become violent.
“You’re looking at a four- to six-month wait to get in with them,” Dellinger learned.
Of 117 facilities that responded to Scripps’ survey, only 46 reported having a psychiatrist on site 24-hours a day to treat patients.

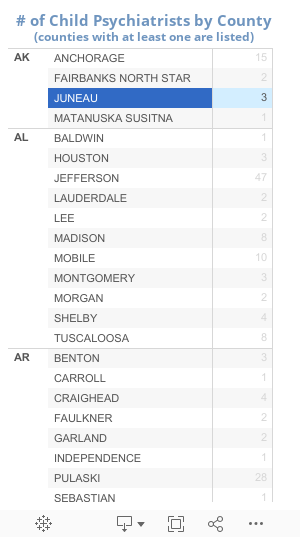
North Carolina is not unique. The American Academy of Child and Adolescent Psychiatrists sets a standard of 47 child psychiatrists for every 100,000 children, but most states average fewer than 17. There are many counties in the country that have none at all.
Efforts to improve mental health care nationwide are in motion, but held up in the legislative churn on Capitol Hill. Since last year, Rep. Tim Murphy, R-Pa., has been pushing legislation aimed at making mental health treatment easier to access. Among the bill’s goals is increasing the number of psychiatric beds by extending Medicaid reimbursement to more hospitals, expanding privacy rules to allow for more communication between doctors and a patients’ caregiver, and extending a government loan forgiveness program to new child and adolescent psychiatrists.
While the bill passed overwhelmingly in the House of Representatives in July, it currently is sidetracked in the Senate by a fight to expand gun rights. Its prospects of passage, according to Murphy’s office, “are murky.”
Murphy’s efforts come at the same time the suicide rate for children is rising. After years of steady decline, the number of children ages 10 to 17 taking their own lives began to quickly rise in 2007. Recently, suicide passed homicide to become the second leading cause of death among teenagers.
As for Ernie and Buffy Goodban, their daughter, Andrea, waited nearly 40 days before finally being admitted to a mental health bed at the University of North Carolina Hospital. After nearly three months of treatment at UNC, the Goodbans were faced with bringing their daughter home or finding longer-term care.
Fearing another long wait for a bed if Andrea was ever again in crisis, the Goodbans chose to place Andrea in a residential treatment center. The facility is more than three hours from their home, making visits difficult and putting an even greater strain on her family.
But bringing their daughter home, the Goodbans said, would almost certainly put their family in danger and lead to another frantic visit to the ER.
“Having to wait all over again,” her father said, “it’d be another nightmare.”
This story was reported by Ross Jones, national investigative correspondent. Angela Hill, national investigative producer, contributed to this report, and Aaron Kessler, national computer-assisted reporting producer, and Maren Machles, national staff intern, also contributed to the report and produced the interactives. Videos were shot and edited by photojournalist Matt Anzur and video editor Vik Narayan. Illustrations were drawn by Sandra Salsbury. You can contact Ross at ross.jones@scripps.com or follow him on Twitter @RossJonesDC.
